What Every Epidemiologist Should Know About Ebola Virus Disease (EVD)
Uncommonly
Reported & Detailed Facts About Ebola Virus Disease From CDC and WHO
1. Period of Infectivity
The incubation period, the time interval from
infection with the virus to onset of symptoms, is 2 to 21 days.
Symptoms may appear anywhere from 2 to 21 days after exposure to
ebolavirus--though 8-10 days is most common.
People are infectious as long as their blood and
secretions contain the virus. For this reason, infected patients
receive close monitoring from medical professionals and receive
laboratory tests to ensure the virus is no longer circulating in
their systems before they return home. When the medical
professionals determine it is okay for the patient to return home,
they are no longer infectious and cannot infect anyone else in their
communities.
Men who have recovered from the illness can still
spread the virus to their partner through their semen for up to 7
weeks after recovery. For this reason, it is important for men to
avoid sexual intercourse for at least 7 weeks after recovery or to
wear condoms if having sexual intercourse during 7 weeks after
recovery.
2. Infection and Transmission
In Africa, fruit bats are believed to be the natural
hosts of Ebola virus. The virus is transmitted from wildlife to
people through contact with infected fruit bats, or through
intermediate hosts, such as monkeys, apes, or pigs that have
themselves become infected through contact with bat saliva or feces.
People may then become infected through contact with
infected animals, either in the process of slaughtering or through
consumption of blood, milk, or raw or undercooked meat.
The virus is then passed from person to person
through direct contact with the blood, secretions or other bodily
fluids of infected persons, or from contact with contaminated
needles or other equipment in the environment.
3.
Preventive Measures
Raising awareness of the risk factors for infection
and the protective measures that should be taken is the only way to
reduce human infection and subsequent deaths. Close unprotected
physical contact with Ebola patients should be avoided. Appropriate
use of gloves and personal protective equipment (including hand
hygiene before putting on, and especially after taking off personal
protective equipment) should be practised when taking care of ill
patients at home. Regular hand washing is required after visiting
patients in hospital, as well as after taking care of patients at
home.
4. Nosocomial Transmission
Almost all transmission of the virus to health-care
workers has been reported when basic infection control measures have
not been observed. Health-care workers caring for any patient should
practice standard precautions. When caring for patients with
suspected or confirmed Ebola virus infection, health-care workers
should apply, in addition to standard precautions, other infection
control measures to avoid any exposure to patients’ blood and body
fluids and with possibly contaminated environments.
5. Burial
Preparation for burial of the bodies of persons who
have died from Ebola virus disease also carries high risks of
transmission of the virus. Those who have died from the disease
should be promptly and safely buried.
6.
Signs and symptoms
Ebola virus is the
cause of a viral hemorrhagic fever disease.
EVD, which has a case fatality rate of up to 90%, is
a severe acute viral illness often characterized by the sudden onset
of fever, intense weakness, muscle pain, headache, nausea and sore
throat. This is followed by vomiting, diarrhoea, impaired kidney and
liver function, and in some cases, both internal and external
bleeding. Laboratory findings frequently include low white blood
cell and platelet counts and elevated liver enzymes.
7.
Diagnosis and treatment
When considering the diagnosis of EVD, other, more
common diseases should not be overlooked; for example, malaria,
typhoid fever, shigellosis,
cholera, leptospirosis, plague,rickettsiosis,
relapsing fever, meningitis, hepatitis and other viral haemorrhagic
fevers.
Definitive diagnosis of EVD is made through
laboratory testing. Because samples from patients are a source of
infection risk for others, testing is conducted under maximum
biological containment conditions.
No vaccine is available, nor is there any specific
treatment. Severely ill patients require intensive supportive care.
Patients are frequently dehydrated and require oral rehydration with
solutions containing electrolytes, or intravenous fluids.
8. What Virus Strain
Is It?
Ebola first appeared in 1976 in 2 simultaneous
outbreaks, in Nzara, Sudan, and in Yambuku, Democratic Republic of
Congo. The latter was in a village situated near the Ebola River,
from which the disease takes its name.
Genus Ebolavirus is 1 of 3 members of the Filoviridae family
(filovirus), along with genus Marburgvirus and genus Cuevavirus.
Genus Ebolavirus comprises 5 distinct species:
►
Bundibugyo ebolavirus (BDBV)
►
Zaire ebolavirus (EBOV)
►
Reston ebolavirus (RESTV)
►
Sudan ebolavirus (SUDV)
►
Taï Forest ebolavirus (TAFV)
BDBV, EBOV, and SUDV have been associated with large
EVD outbreaks in Africa,
whereas RESTV and
TAFV have not. The RESTV species, found
in Philippines and the People’s Republic of China, can infect
humans, but no illness or death in humans from this species has been
reported to date. Samples
taken from patients in this outbreak have tested positive for EBOV.
Genetic analysis of the virus indicates that it is closely related
(97-98% identical) to variants of Ebola virus identified earlier in
the Democratic Republic of the Congo and Gabon.
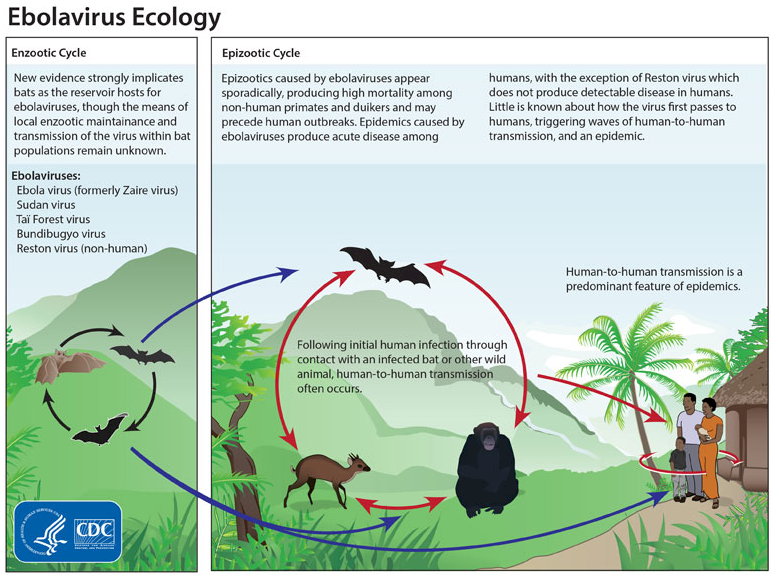
This graphic shows the life cycle of the ebolavirus. Bats
are strongly implicated as both reservoirs and hosts for the
ebolavirus. Of the five identified ebolavirus subtypes, four
are capable of human-to-human transmission. Initial
infections in humans result from contact with an infected
bat or other wild animal. Strict isolation of infected
patients is essential to reduce onward ebolavirus
transmission.
Reprinted from CDC:
http://tinyurl.com/l4bmums |
|
 |
| |
| Ebola
Hemorrhagic Fever Outbreak in Guinea,
Liberia, and
Sierra Leone 2014
Reprinted
from CDC:
http://tinyurl.com/l5mht3y |
|
 |
|