|
|
||||||
|
|
||||||
|
Local Data for Local
Action: |
||||||
|
Authors:
: Jasmine
Soriano, LeeAnn Prebil, Matthew Willis It was a Wednesday morning in January of 2021 and I logged in nervously to the Marin County COVID-19 Vaccination Strategy Meeting and waited for others to virtually arrive. We did this every week; however, this was different because we were in the midst of a COVID-19 tsunami in Marin County due the holidays and colder weather. A perfect storm for respiratory viruses. We were seeing an average of 2 deaths and 100 cases per day. Help was finally here in our fight against COVID-19—vaccines. But, we had a big problem. Demand far outpaced supply. This particular morning, tough decisions had to be made on where our mobile vaccination teams were deployed. Which groups do we focus on in outreach and messaging? Who gets priority? Answers to these questions were shaped by the local epidemiological data our team prepared in lock hand with a coalition of healthcare providers, community-based organizations, school leadership, faith-based leaders, and elected officials. Knowing that our analyses determined who would be offered the vaccine the next day made our impact as epidemiologists clear. At the time, the state of California depended on local health jurisdictions to coordinate distribution of vaccines to a network of local vaccine providers. On a weekly basis, each California county was allocated a certain number of doses. Receiving the full allocation relied on effective use of prior allocations. This model required a locally defined vaccination strategy which made two elements crucial: 1) timely, local data and 2) countywide collaboration.
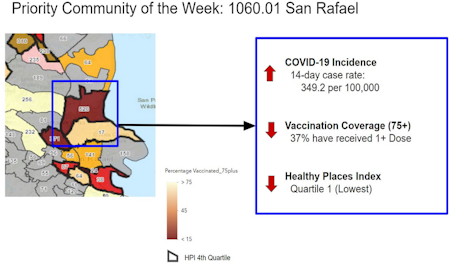
Local data led us to modify national or state guidance for tailored county policies. In January 2021, Marin County limited vaccine availability to residents 75 years or older, despite CDC’s and California’s threshold at 65 years of age. This decision was based on two factors — 1. Marin County’s older age distribution, and 2. Local COVID-19 mortality rates. Our analysis of the association between vaccine status and mortality within our community made this decision clear. For the public, we explained it this way: “Three out of four COVID-19 deaths in Marin are among our residents 75 years or older” and, “In Marin today, a vaccine offered a resident above age 75 is more than 300 times more likely to save a life than a vaccine offered to someone under age 50.” Aligning messaging across the community, with compelling local data and with the buy-in of the countywide vaccine coalition, helped justify a narrower focus when residents of other age groups advocated to their providers and elected leaders. One month into vaccine distribution, Marin had the highest vaccination coverage of residents 75 years and older of any county in the nation, likely contributing to the county’s relatively low cumulative mortality despite our demographic risk profile. Timely data and cross-domain collaboration shaped the COVID-19 vaccination strategy during these Wednesday morning meetings. Each week, we organized vaccination coverage data by census tract, race/ethnicity, age, and income level. We showed community-level COVID-19 burden through case rates, percent positivity, hospitalization, and death rates. We developed a vaccine prioritization system using census tract level COVID-19 case rates, vaccination coverage, and community resource level (using the California Healthy Places Index) to direct vaccine operations in real time. We also showed wait times at vaccination sites, and explored vaccine hesitancy through a public survey.
These data were shared with the public through the Marin County COVID-19 Surveillance webpage. Marin residents were provided with information updated daily they could use to track progress toward our equity goals, understand the rationale for local policies, and make individual health decisions. Communication with the public was bidirectional. We crafted responses to public inquiries about the data and honed our dashboard to ensure clarity of communication. This transparency likely contributed to the community’s trust in government and healthcare providers, and ultimately, high vaccination rates. Our epidemiological work was not routine or fixed. COVID-19 vaccine data was like a river, in ever-changing motion. Gaining access to the state immunization registry was one of many steps in scouring the landscape of useful data sources. As new groups became eligible and new vaccine formulations were added, we developed methods to show vaccine coverage by relevant strata. Population denominators derived from Census Bureau data became puzzles we were tasked to solve. We worked closely with our Information Technology department to develop local data collection systems, and shared tools and ideas with epidemiologists from other jurisdictions. The coalition continued pivoting local vaccination operations based on the nearly real-time data we presented each week. Over time, we saw silos in our health and social safety net systems dissipate through the shared goal of vaccinating our population. We learned that all stakeholders, including community members, share an appetite for data, provided it is translated into culturally relevant and meaningful terms. This understanding has contributed to our standing as one of the most highly vaccinated counties in the nation, for all age and race/ethnicity groups. One frequently cited challenge to a single national vaccination strategy is the diversity of communities across the nation. Most political, demographic, economic and cultural realities are hyper-local, and exert strong influence over vaccine access and uptake. In our experience, using local data to define a coherent strategy ensures more efficient and equitable vaccine uptake.
On those Wednesday
mornings, at the center of a local campaign to save lives through
vaccines, our team felt a unique responsibility to perform excellent
epidemiology. Helping drive public health practice where it matters most,
at the level of community, is a unique reward of a local epidemiologist.
We will carry the lessons from our pandemic response as we face new public
health threats, and our approach to rally around local data as a driving
force for action will be natural. We will make good use of that Wednesday
morning meeting.
■ |
||||||